
Dr Jeannette Wolfe, an academic emergency physician, and Barbara Annis, Founder and CEO of Gender Intelligence Group, share their insights into the worldwide pandemic COVID 19
 Have you ever sat in the passenger seat of a car and pressed down on an imaginary brake because you were increasingly uncomfortable by the driver’s speed and their brazen flirtation with disaster? In the past week, life as we know it has been unprecedentedly disrupted by COVID-19. Right now, we are all riding shotgun and COVID-19 is behind the wheel. The question is, are we all wearing our seatbelts?
Have you ever sat in the passenger seat of a car and pressed down on an imaginary brake because you were increasingly uncomfortable by the driver’s speed and their brazen flirtation with disaster? In the past week, life as we know it has been unprecedentedly disrupted by COVID-19. Right now, we are all riding shotgun and COVID-19 is behind the wheel. The question is, are we all wearing our seatbelts?
So why are a frontline emergency medicine physician and a business CEO teaming together to write about COVID-19? Because we are both experts in how biological sex and gender influence our bodies and behaviour and we realise that the actions people take or don’t take in the next few weeks will heavily impact the overall mortality rates of this virus. So, we think it’s time we have a frank talk about sex, gender and COVID-19.
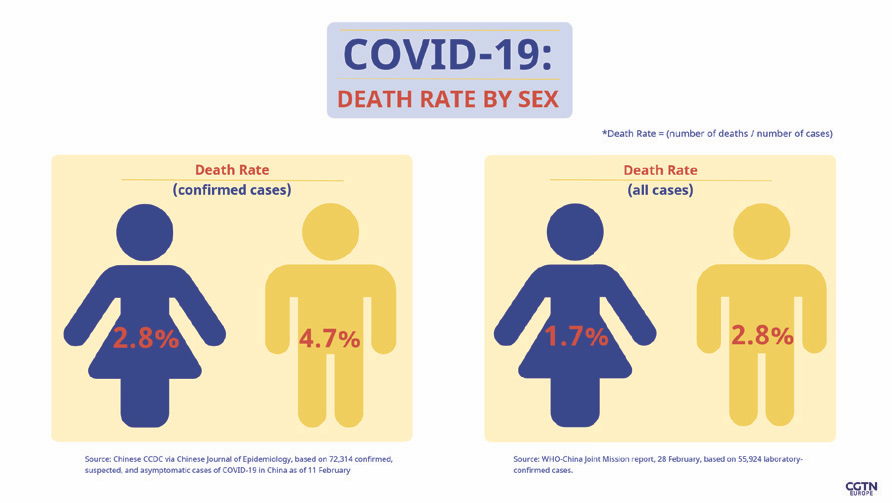
From the data we have so far, physiologically, males appear to be at greater risk of having symptoms, and of dying from COVID-19. In Italy, currently 58 per cent of confirmed cases are male, and in China sources have shown the death rate to be between 2.8 to 4.7 per cent in men versus 1.7 to 2.8 per cent in women. Of note, previous coronavirus outbreaks including the severe acute respiratory syndrome (SARS) and the Middle East respiratory syndrome (MERS) also killed more men. Some of this gap is due to differences in gender-based cultural habits, for example, in China, far more men than women smoke. However, there also appears to be a biological sex-based difference in immunology. Detailed basic science research on SARS showed that after being inoculated with similar amounts of virus, male mice experienced higher viral titers and greater inflammatory changes in their lungs. Importantly, their findings correlated with age. In those at the extreme of age there were no significant differences, but for those in between it was quite pronounced, with a group of middle-aged mice infected with a moderate amount of virus showing a 90 per cent mortality in the males but only a 20 per cent mortality in females.
Sex-based differences in COVID-19 death rates are likely due to both sex chromosomes and hormones. Men and women may share over 98 per cent of the same DNA, but we now know which genes get turned on and off after an environmental trigger like an infection can be quite sex specific. Although we once thought our X- and Y-chromosomes were mostly involved with hormonal reproductive housecleaning tasks, recent research suggests that these chromosomes also contain genes that regulate our immune response and actually influence which genes on other chromosomes get read. Interestingly, there is now evidence that COVID-19 infects lung tissue via attaching to the angiotensin-converting enzyme 2 (ACE2) receptor, and the gene for ACE2 is on the X chromosome. Concerning sex hormones, although both men and women have estrogen, progesterone and testosterone in their bodies, their ratios are sex specifi c. Testosterone can suppress immune responses, while estrogen effects are more complicated and vary depending on circulating levels and interactions with different pathways of the immune system. A recent study showed that when nasal cells infected with a fl u virus were exposed to estrogen, they had smaller viral replication rates, suggesting that compared to women, men might require a smaller viral load to get sick. Plus, men may be at greater risk of dying from COVID-19 because in some cases they may have an overly exuberant infl ammatory response that ends up suffocating their lungs and preventing adequate oxygen exchange. Women may be somewhat protected from this infl ammatory overdrive due to certain estrogenic effects that dampen it. When considering big picture numbers as to who and how many might actually die from this pandemic, our biological sex, however, is probably far less of a factor than how we as a society collectively manage these next few weeks. This is where the ‘gender’ part comes in. In general, women historically tend to be more focused on medical issues, are less likely to take unnecessary health-related risks and are more likely to wash their hands. Now is a good time for us all (and perhaps especially risk – tolerant men) to consider the following:
- Respect this virus. As an emergency medicine physician who has weathered the HIV, SARS, H1N1 and Ebola scares, Dr. Wolfe can say that COVID-19 is a different creature. This virus is very contagious and spreads even before someone is symptomatic. Personal accounts of its impact from Italian medical colleagues are chilling and hint to the chaos that will likely hit our health care systems soon. Fortunately, there are lessons from other pandemics that can help us get ready for COVID-19, such as those learnt over a hundred years ago when the Spanish fl u that killed upwards of 100 million people. During that pandemic, cities that supported aggressive early interventions like voluntary quarantines, school closures and bans on public meetings seemed to avoid a signifi cant bolus of people getting critically ill, compared to communities with less restrictive policies. Social distancing works, and for those of you who may still be muttering, “Yeah, but don’t you think we pulled this trigger just a little too early,” unfortunately the answer is a defi nitive “no”. Once even a small amount of a community gets infected, isolation strategies don’t work as well and the number of people getting sick all at once can quickly exceed the amount of available hospital and intensive care beds. COVID-19 makes things even trickier, however, as it appears that patients who survive have longer recovery times compared to patients with more common types of pneumonia. This creates a double logjam – more sick patients coming in and fewer patients going home. Further confounding things are the very real shortages that have already started happening. By now most people are likely aware of the critical mask shortage. In another time, the idea that hospital administrators would be constructing do-it-yourself masks to protect their frontline workers would have been simply absurd. Yet, we are now in a new reality and this is only the beginning. This is a long domino chain.
- Be a modern-day hero. The heroes of this outbreak will be the ones willing to bunker down into the trenches of their living rooms and sacrifice their everyday conveniences to put the health of their families and the most vulnerable in their communities first. Social isolation will only work if people do it.
- Worship altar of Mr. Clean. In a freakishly timed release, this past December a group of researchers published a data-driven simulation model showing how pandemics might be mitigated by having more travelers at airports simply wash their hands. Their modeling suggested that by increasing hand hygiene at 10 core airports, the risk of a pandemic could be decreased by 37 per cent. Although we can’t roll back the clock and just donate a couple of barrels of hand sanitizer to those airports, there is still great value in deciding right now that having clean hands will be your new super power.
- Besides handwashing, here are five other easy ways to slow COVID-19’s spread: cough into your elbow, clean your cell phone, flush the toilet with the seat down, use hand sanitizer after touching shared public surfaces and… wash your hands again. Importantly, if you have kids at home, remember that your optics matter. What you do, will likely influence whether or not they adopt or discard their own COVID-19 prevention habits.
- Secure a sanctuary. With social distancing guidelines and public closures, many families will find themselves spending an uncomfortable amount of time together over the next many weeks. Cabin fever peppered with real concerns about physical risks and financial uncertainties can be a set up for sparks. Know your limits, and when you need a break separate yourself from those you love. If you don’t have a cough or a fever and live in an area where there is adequate space to safely go outside, get some fresh air and exercise. Otherwise, identify an inside place where you can escape to re-centre. Use technology to your advantage: play a game, listen to some music or download a relaxation app. If things get overwhelming, know the resources to get you or your family members help.
- Use your status. Somewhat ironically, the population most at risk in this pandemic – older men – are also the ones who are making many of the key decisions in how government, business and health care systems are reacting to this crisis. If you are fortunate to be in this group, use your influence wisely. This virus is quickly redefining how we do ‘work’, and policies that are made now will influence not only your own personal exposure risk but also those of your colleagues and employees. For our economy to stay afloat during this uncertain time, you will need to be nimble and creative in ways to keep the population who can work, working. Of note, please pay.
 This is it. COVID-19’s foot is on the gas and we are all in for one wild ride. Click in that seatbelt.
This is it. COVID-19’s foot is on the gas and we are all in for one wild ride. Click in that seatbelt.
Dr Jeannette Wolfe is an academic emergency physician and the host of the podcast Sex and Why Twitter @WolfeJeannette
Barbara Annis, Founder and CEO of gender intelligence group, is a world-renowned expert on Gender, Diversity and Inclusivity. Check out www. genderintelligence.com / or e-mail at bannis@genderintelligence.com